Hi all,
I’m working on the IBM team that is building Chemotherapy Ordering. We’ve been working on identifying necessary data points for our solution that aren’t clearly represented in the current data model, and brainstorming where those points could fit, or how we might extend the model to fit those points.
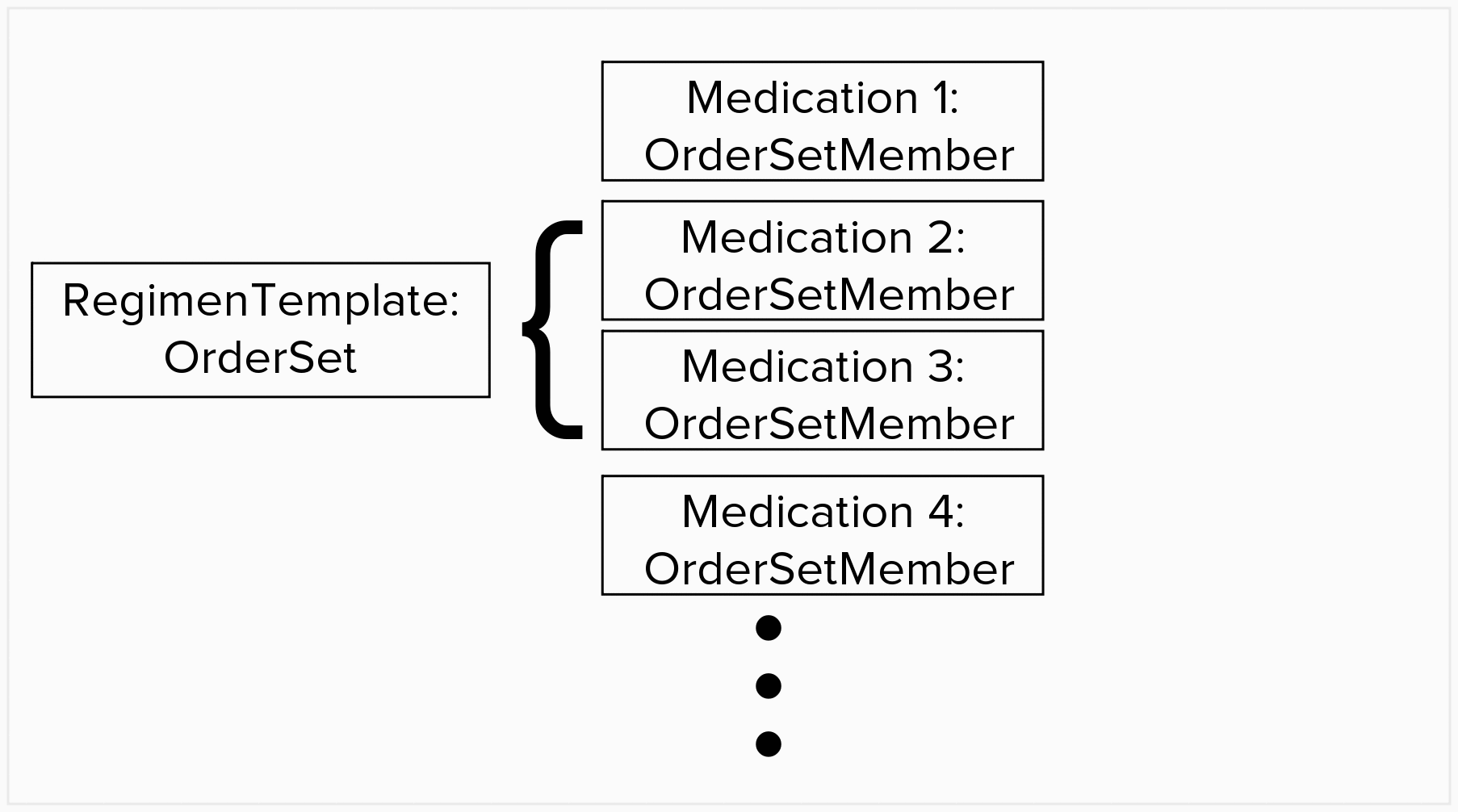
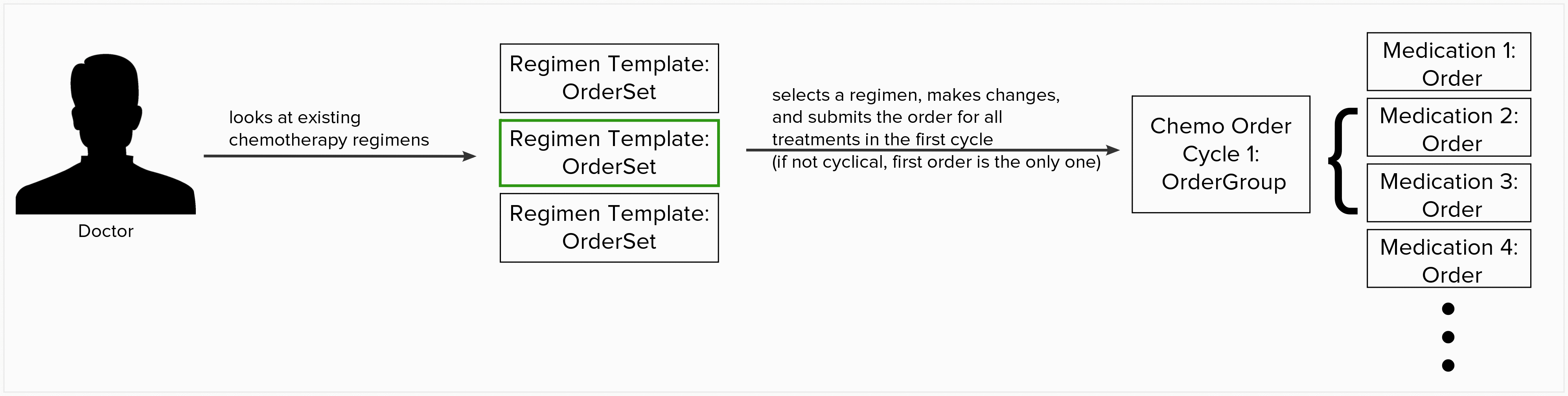
For background, here is how we are planning to model the regimen templates and the chemotherapy orders in the data model:
The missing data points for our use case are:
- OrderSet
- Category (Chemotherapy, HIV, etc)
- Number of cycles typical in the regimen
- Length of cycles typical in the regimen
- OrderGroup
- Cycle number
- Category (Chemotherapy, HIV, etc)
- Number of cycles in the regimen
- Length of the cycles in the regimen
- Prior Order Group
- DrugOrder
- Dosing reduction
- Chemotherapy administration group (Premedication, Chemotherapy, Post Medication)
- Maximum Lifetime Dose
- Drug
- Units for the maximumDailyDose
For OrderSet, we feel that extending the model via attributes makes the most sense. However, Category might be generally useful for indicating what the OrderSet is typically used to treat, so it might make more sense on the OrderSet object.
We also want to extend OrderGroup via attributes. Again, Category might make more sense on the object, but the rest of the fields would be associated via attributes. Our intent behind a Prior Order Group attribute is to link cycles of a regimen together - so Cycle 2 of a patient’s current chemotherapy regimen would link to Cycle 1 of that chemotherapy regimen.
For DrugOrder, we have considered subclassing DrugOrder to create a ChemoOrder class to hold the dosing reduction and chemo administration group information. However, there does seem to be logical fields in the existing data model for the missing info. The chemotherapy administration group could simply be in the orderReason field, but we are not certain if this field is needed for another use. Dosing reduction is a very important data point for chemotherapy ordering. In chemo ordering in Haiti (which is our main focus), when a doctor orders the chemo medication, they don’t calculate the dosage - the dosage calculation is done by the nurse right before administration. However, the doctor may recommend that whatever the calculated dosage, it should be reduced at administration time by a certain percent. The nurse will then calculate the dosage, and after calculation apply the dosing reduction. The concept of a dosing reduction has been explained as specific to the chemotherapy ordering process, and a vital metric to capture and display to the nurse and doctor and possibly use in future orders and calculations. According to this wiki page, dosing reduction seems like it could be serialized in the dosingInstructions field in DrugOrder.
Maximum lifetime dose is being discussed here - Maximum lifetime dose of a particular drug or class of drugs
A design call is being held this afternoon to discuss these decisions, but any guidance is appreciated here as well!
FYI: @mseaton @ddesimone @burke @darius @ilewis
